

Week 5 Assignment 1: Hypertension Management Annotated Study Guide
Week 5 Assignment 1: Hypertension Management Annotated Study Guide
Value: Complete/Incomplete (100 points is Complete and 0 is Incomplete)
Due: Day 7
Grading Category: Other Assignments
Overview
In this assignment, you will complete the following Annotated Study Guide. The study guide is based on the content from this module and is to be completed as you go through your learning material for this module.
It is strongly suggested that you complete this assignment to better prepare for upcoming assignments and exams. This tool will make a handy reference as you go forward in your practice and career.
Instructions
- Download the Hypertension Management Annotated Study Guide (Word) before you begin your week’s assigned geriatric assessment assigned readings.
- Review the study guide for topics that will be of particular importance during your reading, and type notes from your reading into the guide to annotate it.
- Save your final file with your name and assignment title, then follow the instructions to submit your study guide file.
- Use this study guide for yourself to study for the course exams and to review for your boards.
Please refer to the Grading Rubric for details on how this activity will be graded.
To Submit Your Assignment:
- Select the Add Submissions button.
- Drag or upload your files to the File Picker.
- Select Save Changes.
Submission status
| Submission status | Submitted for grading | ||
|---|---|---|---|
| Grading status | Graded | ||
| Time remaining | Assignment was submitted 3 days 10 hours early | ||
| Last modified | Thursday, 2 February 2023, 12:59 PM | ||
| File submissions |
|
||
| Submission comments |
Comments (0)
|
Annotated Study Guide for Hypertension Management
Instructions
Complete/Incomplete
Due Day 7
Each of the hypertension management topics you are responsible for knowing have been collected in this study guide. To help recall and master this material, you will annotate each topic in this study guide with notes, thoughts, and/or images as you perform the required readings at the start of this week. There will be prompts for each topic, but do not consider yourself constrained by these, as long as each topic is annotated in some way.
This assignment will be marked complete and receive full credit if most or all of the topics have been annotated. Your assignment will most likely not receive feedback since the value of this assignment is in its creation (taking notes while reading facilitates active learning which, in turn, promotes better recall) and as a study aid for class exams.
Hypertension Management Topics
Hypertension is
- the most common risk factor for MI and stroke
- Strong contributor to heart disease, CHF, Kidney disease
- Modifiable risk factor for premature cardiac disease
- Smoking
- Dyslipidemia
- DM
Notes:
Blood pressure is
- the major determinant in the reduction of CV risk
Notes:
Complications associated with hypertension are
- LVH
- HF
- Stroke- ischemic and hemorrhagic
- Ischemic heart disease
- MI
- CKD
Notes:
HTN Stats (CDC, 2016)
- Approximately 1 of 3 adults in America (70 million people) have hypertension.
- 54% of those have their blood pressure under control.
- High blood pressure costs the nation $48.6 billion each year.
- 5% of adults are affected by high blood pressure, half of them have it under control
Notes:
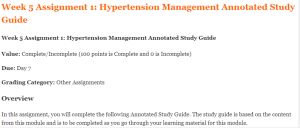
Hypertension prevalence
SOURCE: https://www.healthypeople.gov/2020/topics-objectives/topic/heart-disease-and-stroke
Notes: (How has this map changed since 2011?)
Healthy People 2020
- Visit the HP 2020 progress review
- Present your key thoughts after reviewing slides 6, 7, and 24 – 31.
Key thoughts:
AHA 2017 guidelines for hypertension
- Look at the US Preventative Task force for who, when, and how often you should be screening for HTN.
- USPSTF
- Annual screening: Adults over the age of 40
- High risk
- 130-139/80-8
- Obese
- African American
Notes:
Risk factors for primary HTN
- Age
- Obesity
- Family Hx (2x as common with hypertensive parent)
- Race – African American
- High sodium diet
- Excessive ETOH
- DM
- Dyslipidemia
Notes:
Contributing factors for secondary HTN
(Annotate table to reinforce understanding and recall)
| ● Prescription/ OTC medications:
● Oral contraceptives ● Chronic NSAID use ● TCA, SSRI ● Glucocorticoids ● Decongestants – pseudoephedrine ● Weight loss medications ● Stimulants or illicit drugs ● Renal Disease ● Renal artery stenosis ● CKD |
● Hyperaldosteronism
● Hypertension ● Unexplained hypokalemia ● Metabolic alkalosis ● Obstructive sleep apnea ● Pheochromocytoma – paroxysmal HTN ● Cushing’s syndrome ● Thyroid disorders ● Pregnancy ● Coarctation of the aorta |
Be familiar with the complications of HTN
(Annotate table)
| ● LVH
● CHF ● CAD ● MI ● Sudden Death ● Aortic Dissection ● CVD |
● Proteinuria
● Renal Insufficiency ● Atherosclerosis ● Retinopathy ● Decline in function- Vascular Dementia, Alzheimer’s Dx |
Think about the clinical presentation of HTN
- Often initially not noticed- Preventative Screening imperative
- Symptoms usually occur as consequences of end organ damage – stroke, renal dx, retinopathy, aortic dissection, sequelae of LVF
- 2nd HTN – usually present with s/s consistent with the underlying cause
Notes:
Understand the following HTN information
- Identify target organ damage
- Identify signs of secondary HTN
- Identify reversible exacerbating factors
- Develop baseline to document progression
Notes:
Your assessment should include at a minimum
(Annotate table)
| ● Aggravating factors:
● Medications ● ETOH ● Diet ● Duration: ● Last known normal blood pressure ● Previous attempts at treatment ● Medications ● Presence of risk factors for CV disease |
● Smoking
● DM ● Dyslipidemia ● Physical inactivity ● Family History ● Sleep Apnea ● Snoring ● Daytime somnolence ● Psychosocial Factors |
Look for signs / Sx of target organ damage
- Heart: Chest pain, palpitations, activity intolerance, etc.
- Brain: dizziness, confusion, transient loss of function
- Kidneys: history of renal disease
- Peripheral arterial disease: intermittent claudication
- Retinopathy: visual disturbances
Notes:
Review Metabolic Syndrome
- 3 or more of the following:
- Abdominal obesity: Waist circumference >40” men >35” women
- Glucose intolerance: Fasting glucose >110
- High Triglycerides: >150
- HTN : >130/85
- Low HDL: <40
Notes:
Important aspects of the PE
- Accurate BP – 2 readings
- Height/Weight/BMI
- Vascular Effects:
- Retinal exam: Arterial narrowing, AV nicking, exudate, hemorrhage, papilledema
- Auscultate for carotid, femoral, renal artery, abd bruits
- Thyromegaly, nodules
Notes:
Target organ damage & secondary causes of HTN
- Derm: Signs of Cushing’s –
Cause of secondary HTN (striae and hirsutism)
Notes:
- Cardio-Resp: Signs of Heart Failure, Aortic insufficiency
- Rales, murmurs, tachycardia, S3, S4, lifts, heaves, displaced PMI, edema
- Abd: masses, bruits, pulsation
Notes:
- Neuro: focal deficits, h/o TIA or past stroke, cognitive impairment, visual field cuts
- Peripheral Vascular
- Femoral bruits
- Femoral pulses (Delayed or absent in aortic coarctation)
- Symmetrical pulses
- Lower extremity shin hair loss (shiny)
- LE edema
Notes:
- HEENT
- Retinal Exam – Arteriole narrowing, AV nicking, exudate, hemorrhage, papilledema
- Oral Exam – Sleep Apnea
- Palpate Thyroid
- Carotid Bruits
- Neck vein distension
Notes:
Week 5 Assignment 1: Hypertension Management Annotated Study Guide Reference images
Go to Uptodate and search on ocular effects of hypertension to find an article with the following images:
- Cotton wool spots ocular effects of hypertension–view images
- Hypertensive retinopathy
Notes:
Diagnostics to understand when treating hypertension
- Electrolytes
- Creatinine
- Fasting glucose
- Urinalysis
- Lipid profile
- Abnormal EKG (LVH)
- Echocardiogram (ejection fraction)
Notes:
Pregnant Women
- ACE-I/ARB are contraindicated
- Treatment of HTN
- Methyldopa
- Beta blockers
- Vasodilators
Notes:
African Americans
- Prevalence and severity of HTN is elevated
- Generally respond best to Thiazide and CCB rather than ACE-I, monotherapy recommended for improved response to treatment
- Angioedema with ACE-I occurs 2-4x more frequently
Notes:
Lifestyle Modifications
- Review Dash diet
- Weight Loss: ca 1 mm Hg for every 1 pound
- Decrease ETOH
- Women – 1 drink/day women
- Men – 2 drinks/day
- Aerobic Exercise-30 min most days
- Smoking Cessation
- Stress Reduction
- Yoga or meditation
- Muscle relaxation
Notes:
Treatment goals
Review when you should initiate treatment and what your goals are.
- Non-black population (including diabetics):
- Thiazide, CCB, ACE or ARB
- Black population (including diabetics)
- Thiazide or CCB
- Age >18 years w/CKD
- ACE or ARB
Notes:
Thiazide diuretics
- Act by decreasing blood volume/cardiac output
- Decrease peripheral resistance during chronic therapy
- No added benefit of increasing HCTZ higher than 25mg daily – add 2nd agent
- Drug of choice for pts with no comorbidities, African Americans, obese individuals and elderly
Notes:
Side Effects/Precautions
- Hypokalemia
- Hyponatremia
- Hyperglycemia
- Hyperuricemia
- Hyperlipidemia
- Not safe in renal and hepatic insuff
- Favorable – Osteoporosis
Notes:
Angiotensin Converting Enzyme Inhibitors (ACE-I)
- “-pril”
- Block conversion from Angiotensin I to angiotensin II
- First line therapy:
- HF or LV dysfunction (Reverse remodeling)
- DM
- Proteinuric kidney disease (renal protective)
- Absolutely Contraindicated in Pregnancy/Breast feeding
- African Americans are more prone to angioedema
- Can occur months to years after starting
- ACE angioedema not a normal allergic reaction
- Treatment is removal of drug and supportive care (airway management)
- Cough (dry and irritating) – 5 to 20%
- More common in women and black patients
- Should stop within 4 days when medication stopped
- Hyperkalemia (5% of patients)
- Renal Insufficiency (Baseline Serum Creatinine <3.0 mg/dl is safe)
- Hypotension (Restart at half dose)
Notes:
Angiotensin II Receptor Blockers
- Patients who do not tolerate an ACE-I
- “- sartan”
- Relative contraindication:
- Previous angioedema with ACE
- 2% will have reaction with ARB as well
- In general do not co administer with ACE
- Only benefit with late stage CHF
- Peak effect 4-6 weeks
- Proteinuria control is equal to ACE-I
Notes:
Calcium Channel Blockers (CCB)
- Myocardial (non-dihydropiridine) and vascular smooth muscle relaxation
- Dihydropyridines – Amlodipine (Norvasc)
- Peripheral vasculature
- Adverse Effects: Peripheral Edema
- Women
- Doses >5 mg
- Adding Ace decreases edema
- Non-Dihydropyridines – Diltiazem, Verapamil
- Negative inotrope
- Peripheral vasculature and cardiac tissue
- Slow AV node conduction
- Rate control
- Reynaud’s Favorable
Notes:
CCB adverse effects
- Peripheral edema
- Hypotension
- Flushing
- Nasal congestion
- Tachycardia
- Dizziness
- Nausea
- Nervousness
- Bowel Changes/constipation
Notes:
Management for older adults
- Thiazide diuretic decrease morbidity and mortality in CVA, CHF, MI
- Observe closely for:
- Dehydration
- Orthostatic hypotension
- Hypokalemia
- Start low and go slow – prevent falls
Notes:
General management
- Return one month after starting agent
- Improves compliance
- Maximize compliance
- Work with patients to reduce adverse effects
- Pt education on what to look for
- Switch to another agent if necessary
- Work with patients to reduce adverse effects
Notes:
General treatment contraindications
Make notes for each contraindication to reinforce your recall:
| AHA, ACC and CDC 2013 Suggested HTN Drug choice by medical condition | Drug | Notes |
| Systolic HF | ACE or ARB, BB, Diuretic | |
| Post MI | ACE or ARB, BB | |
| Proteinuric CKD | ACE or ARB | |
| Angina | BB, CCB | |
| Afib/flutter rate control | BB, nondihydropyridine CCB |
General treatment contraindications
Make notes for each contraindication to reinforce your recall
| Contraindication | Drug | Notes |
| Angioedema | ACE Inhibitor | |
| Bronchospasm | Beta Blocker | |
| Pregnancy | ACE or ARB | |
| Heart Block | BB or nonhydropyridine CCB |
Lopes Write Policy
For assignments that need to be submitted to Lopes Write, please be sure you have received your report and Similarity Index (SI) percentage BEFORE you do a “final submit” to me.
Once you have received your report, please review it. This report will show you grammatical, punctuation, and spelling errors that can easily be fixed. Take the extra few minutes to review instead of getting counted off for these mistakes.
Review your similarities. Did you forget to cite something? Did you not paraphrase well enough? Is your paper made up of someone else’s thoughts more than your own?
Visit the Writing Center in the Student Success Center, under the Resources tab in LoudCloud for tips on improving your paper and SI score.
Late Policy
The university’s policy on late assignments is 10% penalty PER DAY LATE. This also applies to late DQ replies.
Please communicate with me if you anticipate having to submit an assignment late. I am happy to be flexible, with advance notice. We may be able to work out an extension based on extenuating circumstances.
If you do not communicate with me before submitting an assignment late, the GCU late policy will be in effect.
I do not accept assignments that are two or more weeks late unless we have worked out an extension.
As per policy, no assignments are accepted after the last day of class. Any assignment submitted after midnight on the last day of class will not be accepted for grading.
Click here to ORDER an A++ paper from our Verified MASTERS and DOCTORATE WRITERS:
Communication
Communication is so very important. There are multiple ways to communicate with me:
Questions to Instructor Forum: This is a great place to ask course content or assignment questions. If you have a question, there is a good chance one of your peers does as well. This is a public forum for the class.
Individual Forum: This is a private forum to ask me questions or send me messages. This will be checked at least once every 24 hours.
Important information for writing discussion questions and participation
Welcome to class
Hello class and welcome to the class and I will be your instructor for this course. This is a -week course and requires a lot of time commitment, organization, and a high level of dedication. Please use the class syllabus to guide you through all the assignments required for the course. I have also attached the classroom policies to this announcement to know your expectations for this course. Please review this document carefully and ask me any questions if you do. You could email me at any time or send me a message via the “message” icon in halo if you need to contact me. I check my email regularly, so you should get a response within 24 hours. If you have not heard from me within 24 hours and need to contact me urgently, please send a follow up text to
I strongly encourage that you do not wait until the very last minute to complete your assignments. Your assignments in weeks 4 and 5 require early planning as you would need to present a teaching plan and interview a community health provider. I advise you look at the requirements for these assignments at the beginning of the course and plan accordingly. I have posted the YouTube link that explains all the class assignments in detail. It is required that you watch this 32-minute video as the assignments from week 3 through 5 require that you follow the instructions to the letter to succeed. Failure to complete these assignments according to instructions might lead to a zero. After watching the video, please schedule a one-on-one with me to discuss your topic for your project by the second week of class. Use this link to schedule a 15-minute session. Please, call me at the time of your appointment on my number. Please note that I will NOT call you.
Please, be advised I do NOT accept any assignments by email. If you are having technical issues with uploading an assignment, contact the technical department and inform me of the issue. If you have any issues that would prevent you from getting your assignments to me by the deadline, please inform me to request a possible extension. Note that working fulltime or overtime is no excuse for late assignments. There is a 5%-point deduction for every day your assignment is late. This only applies to approved extensions. Late assignments will not be accepted.
If you think you would be needing accommodations due to any reasons, please contact the appropriate department to request accommodations.
Plagiarism is highly prohibited. Please ensure you are citing your sources correctly using APA 7th edition. All assignments including discussion posts should be formatted in APA with the appropriate spacing, font, margin, and indents. Any papers not well formatted would be returned back to you, hence, I advise you review APA formatting style. I have attached a sample paper in APA format and will also post sample discussion responses in subsequent announcements.
Your initial discussion post should be a minimum of 200 words and response posts should be a minimum of 150 words. Be advised that I grade based on quality and not necessarily the number of words you post. A minimum of TWO references should be used for your initial post. For your response post, you do not need references as personal experiences would count as response posts. If you however cite anything from the literature for your response post, it is required that you cite your reference. You should include a minimum of THREE references for papers in this course. Please note that references should be no more than 5 years old except recommended as a resource for the class. Furthermore, for each discussion board question, you need ONE initial substantive response and TWO substantive responses to either your classmates or your instructor for a total of THREE responses. There are TWO discussion questions each week, hence, you need a total minimum of SIX discussion posts for each week. I usually post a discussion question each week. You could also respond to these as it would count towards your required SIX discussion posts for the week.
I understand this is a lot of information to cover in 5 weeks, however, the Bible says in Philippians 4:13 that we can do all things through Christ that strengthens us. Even in times like this, we are encouraged by God’s word that we have that ability in us to succeed with His strength. I pray that each and every one of you receives strength for this course and life generally as we navigate through this pandemic that is shaking our world today. Relax and enjoy the course!
Hi Class,
Please read through the following information on writing a Discussion question response and participation posts.
Contact me if you have any questions.
Important information on Writing a Discussion Question
- Your response needs to be a minimum of 150 words (not including your list of references)
- There needs to be at least TWO references with ONE being a peer reviewed professional journal article.
- Include in-text citations in your response
- Do not include quotes—instead summarize and paraphrase the information
- Follow APA-7th edition
- Points will be deducted if the above is not followed
Participation –replies to your classmates or instructor
- A minimum of 6 responses per week, on at least 3 days of the week.
- Each response needs at least ONE reference with citations—best if it is a peer reviewed journal article
- Each response needs to be at least 75 words in length (does not include your list of references)
- Responses need to be substantive by bringing information to the discussion or further enhance the discussion. Responses of “I agree” or “great post” does not count for the word count.
- Follow APA 7th edition
- Points will be deducted if the above is not followed
- Remember to use and follow APA-7th edition for all weekly assignments, discussion questions, and participation points.
- Here are some helpful links
- Student paper example
- Citing Sources
- The Writing Center is a great resource